

Medical coding audits are an essential part of the healthcare industry, as they help to ensure that organizations are accurately coding their services. There are numerous benefits to conducting external medical coding audits including ensuring that medical providers are compliant with coding regulations.
The goal is to identify any errors and to help medical practices and physicians improve their coding and billing practices. Auditors can provide feedback to help them understand and correct any coding errors.
These are conducted by experienced auditors who are knowledgeable about third-party regulations. Revenue managers are playing on an uneven playing field with payers. But it doesn’t have to be that way. Subject matter experts exist to help healthcare groups to get paid what they deserve by providing them with practical solutions and services tailored to their needs.
A recent study showed that organizations 34 % base their need of performing an audit on the OIG work plan and 17% on organizational mandates or policy. Shouldn’t audits be based on data and not on internal policies? When we review the data what is it telling us?
Let’s review what the data is telling us regarding productivity, denials, and trends.
Measuring Staff Productivity
Medical coding roles have changed over the years, and the productivity standards overhaul is far behind schedule. Now, with the staff shortages and high volume of claims, the time has come for organizations to set new productivity standards. At the same time, health care reform, particularly the reforms in reimbursement, has expanded the data elements a medical coder must account for and capture in coding form, adversely affecting coding productivity.
Setting standards for productivity is important but is much more complex than simply how many charts a medical coder is abstracting in an hour. The truth is that the mental processes involved in the coding process are almost never considered when measuring coder performance, and when it comes to accuracy, as they say, quantity does not equal quality. Insurers use coding to compute payments, so coding productivity standards have a direct impact on medical professionals’ profit margins.
To remain profitable, hospitals and physician practices require timely payments, and that requires that coders be productive, effective, and accurate. If facility coders take on professional-fee billing, then it is necessary to revisit the standards of productivity they are held to. Best practices for directors and managers are to define coding performance standards explicitly, but they should also take into account elements unique to their environments that impact the productivity measures of their own coding teams.
Health Information Management (HIM) directors can speak dollars and cents with their CFOs in discussions surrounding coder productivity; staffing; unbillable management; and building critical relationships with the physician workforce, patient care administration, clinical documentation improvement (CDI), and all departments that are directly related to the timely, accurate, consistent, and thorough documentation of medical records, and the effect they have on revenue and data integrity. Using user-friendly, real-time reporting dashboards, HIM directors can capture coder performance, perform causal analyses, and identify opportunities for improvement.
For coders, productivity typically refers to the number of surgical/procedural or evaluation and management (E/M) codes encountered, records reviewed, providers trained, remedial plan issues, etc. The main measure for evaluating coder performance for the state code charts — the number of codes a day, per week, or per pay period.

When productivity is related to coders, it is measured in terms of the actual time spent on tasks, utilization of internal and external sources, and required technologies.
Review the full productivity study by Decision Health
Utilize your Staff Efficiently
There are a number of benefits to conducting thorough job assignments to determine the coder on staff most appropriate, but it is important to note that there are times when a coder is better suited for extra tasks. If you have a coder that is being pulled out of helping out with non-coding-related tasks, you might want to reassess their workflow. If the workflow is not clear, then your coding team is going to be spending time doing tasks that are not beneficial to the organization.
To improve the productivity of your medical coding team, you must create workflows that decrease the number of overhead tasks, and work collaboratively with your team members to identify bottlenecks in their workflows and mitigate these bottlenecks so time is freed up to perform high-value tasks. If you are looking for ways to increase productivity as a medical coder, or any other team member who is spending time on activities that are not producing a high-value output, keep reading.
Code Interceptor was created to help increase the efficiency and productivity of your staff while helping them stay current with the latest coding guidelines. With constant changes in the healthcare industry, it is essential that your coders keep current on the latest updates related to coding in the CPT and ICD-10 code sets. If you have not been tracking performance before, Spark Advisory Network offers data reviews and onsite productivity improvement assessments.
Denial Trends
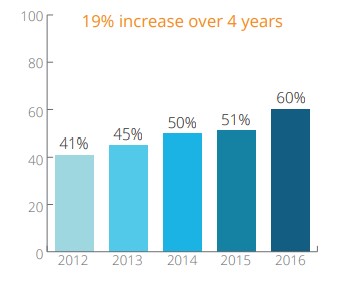
Data shows that 24% of organizations do not follow recommendations from their internal and external audit reviews, which will increase the possibility of a loss in revenue, increasing denial rates, and the additional risk of a payer audit with the potential for fines. There is also research that shows there was a 19% increase in coders performing appeals for denials from 2012 to 2016. It’s important to track the non-coding related tasks your coders are performing to analyze their effectiveness as coders as well as if other roles are needing education and improvement in communication with the coding teams.

Technology Enabled Coding
“CACs (Computer-assisted Coding) can do much of the heavy lifting for coders, who must then only review coded information”, says Melanie Endicott, senior director for HIM practice excellence, coding, and CDI product development at AHIMA.
A survey of medical practices shows that 38% of organizations utilize Computer Assisted Coding (CAC) Software. Although CAC cannot replace the human brain and true analytical professionals, it can improve the process. Computer-assisted coding (CAC) has helped improve the efficiency of a coder’s workflow and decrease the number of times that the coder has to revise the chart in order to correct data quality errors. Because CAC requires a human coder to review each patient’s chart, healthcare organizations using it will have to hire more coding staff as their charts become more numerous. If then only 38% are using CAC in coding processes, wouldn’t it make sense to have an expert in coding and CAC come in and review the accuracy at least quarterly?
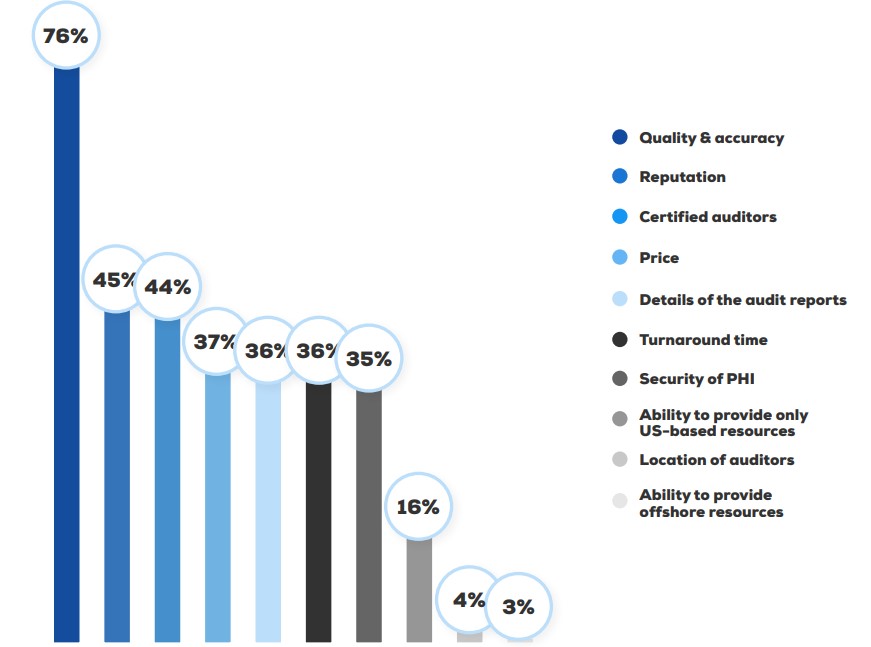
What are organizations looking for in an external auditing vendor?
Annual Compliance &
Auditing Benchmark Report Healthicity
Benefits of an External Audit
Establishing regular medical coding audits will help you to get high ROI, as well as keep the best coding practices in place to grow the healthcare organization. Outsourcing a code audit to medical coding companies like Oncospark can help organizations get a more objective assessment of their coding practices. With their consultation and auditing services, organizations get support and an in-depth examination that helps them improve the accuracy of their claims and optimize coding processes.
Frequent in-house or out-sourced audits provide a quality assurance process that helps organizations achieve appropriate reimbursements and maintain regulatory compliance. An important distinction between internal and external audits of billing is that an external audit can be more objective, with results that are more likely to be accepted by providers and other stakeholders. An internal audit can be conducted periodically by coders trained to review the medical records or a practitioner trained in auditing coding and compliance.
How frequently to conduct medical coding audits may depend on any number of factors, including the size of the organization, turnover rate, and regulatory updates. These audits serve as preventative measures, so organizations can identify errors in billing and compliance early before they cause larger problems. With periodic medical coding audits, providers can comply with compliance standards, lower denials, and avoid investigation and penalties.
By performing a coding audit every month (or quarter), healthcare organizations identify errors they can correct, leading to increased revenues/compliance. Armed with monthly audit insights, healthcare organizations are more quickly able to identify areas of improvement for clinical documentation, thereby improving overall coding processes. Afterward, healthcare organizations can adapt their coding processes to prevent future harm to their bottom lines. An external coding audit provides providers with an objective, third-party evaluation of their medical coding procedures and policies.
Moving from an annual to a regular, external coding audit schedule adds costs to healthcare providers’ organizations. While internal audits are important to the organization, external audits improve the likelihood that potential compliance risks will be identified. More importantly, audits on medical billing may identify inappropriate billing practices, either due to errors or fraud.
Prospective coding and billing audits can help large organizations save time on the reworking of claims rejected by payers. Not only do coding audits uncover emerging laws for you, but they also help keep you up-to-date on emerging payer regulations and other frequently occurring challenges faced by physician practices. One major benefit of a prospective audit is that you get to see your office’s state-of-the-art coding practices in action before a single inappropriate claim is submitted.
Auditing helps to keep your operations running at peak efficiency, as manually coded health care is a massive pain point for providers all over. Outsourcing the medical chart auditing as well as coding services allows hospitals and other healthcare practices to cut costs, such as the HR aspects of running, hiring, training, and scheduling the in-house coding departments. Similar to in-house audits for coding staff, outside audits identify opportunities for training and process improvements, which ultimately results in a more effective coding department with fewer errors, fewer denials, and correct claims processing.